SUPPLEMENTARY
MATERIALS
Construction of an open-access QT database for detecting the proarrhythmic potential of marketed drugs: ECG-ViEW
Authors: MY Park, MS,
D Yoon, MD, MS, NK Choi, PhD, J Lee, MD, MS, K
Lee, PhD,
HS Lim,
BJ Park, MD, MPH, PhD,
JH Kim, MD, PhD, RW Park, MD, PhD
DATA
EXTRACTION
Parameter extraction from ECG printouts using OCR software
Graphic software was used to
pre-process scanned ECG printouts. Gray-scale
conversion, cropping to text area, and removing background dirt by adjusting the
brightness level were conducted in sequence. Image pre-processing of all
the images was
performed automatically using a macro function of the graphic software. OCR
software was used to extract parameters from a pre-processed
image. OCR is
the electronic translation widely used for
converting books and documents into electronic files, to
computerize a record-keeping system in an office, or to publish text on a
website. The macro function of the OCR software enabled the
recognition of ECG readings from the ECG images into text files automatically.
Incorrect cases were collected, and falsely recognized characters in the images
were trained by using the character-training function provided by the
OCR software. We developed a Java-based text-parsing
software that parsed ECG parameters from the recognized texts files. Overall
processing is illustrated in the following diagram.
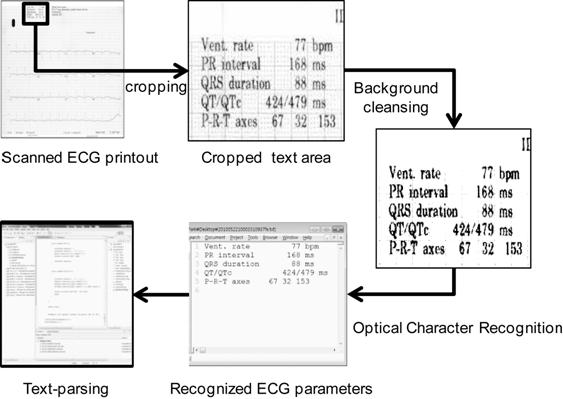
<Overall process to extract ECG parameters from scanned ECG
printout>
Web-parsing
software
for parameter extraction
from ECG management system
We developed Java-based web-parsing
software that sends
a request to the web viewer of the ECG management system. Returned
PDF files containing ECG parameters and ECG waveforms from the ECG management system were saved into a file folder. All the stored ECG
records in the ECG management system were retrieved and saved as PDF files by
sequentially iterating the request and saving
the loop for all
patients who ever visited the
subject hospital. A
pause of 0.5 sec was placed between sequential requests to prevent unexpected
shut down or breakdown of the ECG management system due
to overload. A 5-minute pause
every 55 minutes and a 30-minute pause
every day were also included.
A
centralized ECG management system should always
be
running without a pause. Thus, extracting all stored ECG records
may hinder the performance of the system or can cause a breakdown.
We tried to minimize the burden on the system by pausing
at
various intervals before the next request to the ECG management system. The
stability or performance of the ECG management systems of individual
hospitals may vary. Thus, our strategy to pause between sequential requests
must be adapted to the individual system. We believe that the suggested pause
between requests is sufficient.
De-identification of data
<Removed
diagnoses from the database, which are highly stigmatized >
|
ICD-10 codes
|
Descriptions
|
|
|
A50-A64
|
Infections with a predominantly sexual mode of transmission
|
|
|
B20-B24
|
Human immunodeficiency virus [HIV] disease
|
|
F10-F19
|
Mental and behavioural disorders due to psychoactive substance
use
|
|
F52
|
Sexual dysfunction, not caused by organic disorder or disease
|
|
F65
|
Disorders of sexual preference
|
|
F70-F79
|
Mental retardation
|
|
N46
|
Male infertility
|
|
N48
|
Other disorders of penis
|
|
N50
|
Other disorders of male genital organs
|
|
O00-O08
|
Pregnancy with abortive outcome
|
|
O30-O48
|
Maternal care related to the fetus and amniotic cavity and possible
delivery problems
|
|
Q00-Q07
|
Congenital malformations of the nervous system
|
|
Q10-Q18
|
Congenital malformations of eye, ear, face and neck
|
|
Q20-Q28
|
Congenital malformations of the circulatory system
|
|
Q30-Q34
|
Congenital malformations of the respiratory system
|
|
Q35-Q37
|
Cleft lip and cleft palate
|
|
Q38-Q45
|
Other congenital malformations of the digestive system
|
|
Q50-Q56
|
Congenital malformations of genital organs
|
|
Q60-Q64
|
Congenital malformations of the urinary system
|
|
Q65-Q79
|
Congenital malformations and deformations of the musculoskeletal
system
|
|
Q80-Q89
|
Other congenital malformations
|
|
Q90-Q99
|
Chromosomal abnormalities, not elsewhere classified
|
|
T73
|
Effects of other deprivation
|
|
T74
|
Maltreatment syndromes
|
|
X60-X84
|
Intentional self-harm
|
|
X85-Y09
|
Assault
|
|
Z72
|
Problems related to lifestyle
|
|
Z80-Z99
|
Persons with potential health hazards related to family and personal
history and certain conditions influencing health status
|
|
|
|
|
|
Software
tools
We
used Eclipse 3.2.2 (IBM, Riverton, NJ) as a Java programming tool for
the web-parsing and text-parsing software. MS-SQL 2000 (Microsoft,
Redmond, WA) was used as the database-management system. Paint Shop Pro
8 (Jasc Software, Eden Prairie, MN) was used to
pre-process the
scanned ECG images. ABBYY FineReader 11.0 (ABBYY Software, Moscow, Russia) was used for
OCR.
CHARACTERISTICS OF ECG-ViEW
Characteristics
of ECGs in ECG-ViEW. The QT database contains 710,369 evaluable ECG records
from 371,401 patients over a 17-year study period,
including
508,978 patient years. The
average
observation period was 502 ± 1,008 days, and the patients had an average of
1.9 ECGs. Most patients had
only one ECG; the interval between the consecutive ECGs was decreased as the number of ECGs/patient increased. The interval between ECG dates in patients who had more than two ECGs was 544.7 ± 813.3 days.
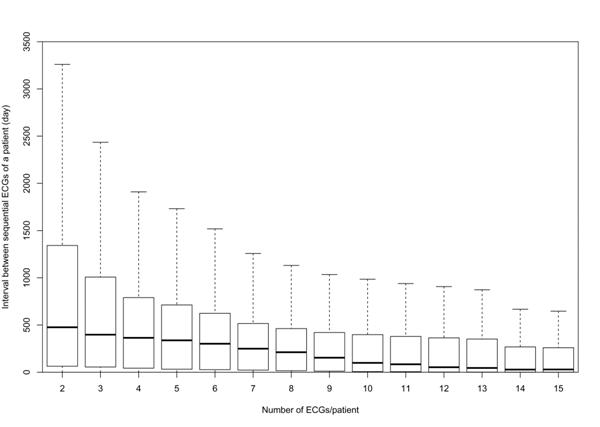
<The intervals between consecutive ECG measurements by the number
of ECGs recorded>
The mean age of patients was 42.4
years, and 50.0%
of patients were female. Most of the study population was
Korean (99.1%). Age-adjusted CCI values
of 5–6 were
most prevalent (34.3%). The average QT and QTc (by Bazett's
formula) were 383.2 ± 41.0 and 414.9 ± 26.3
ms for males, and 387.3 ± 42.2 and 423.9
± 27.1 ms for females,
respectively.
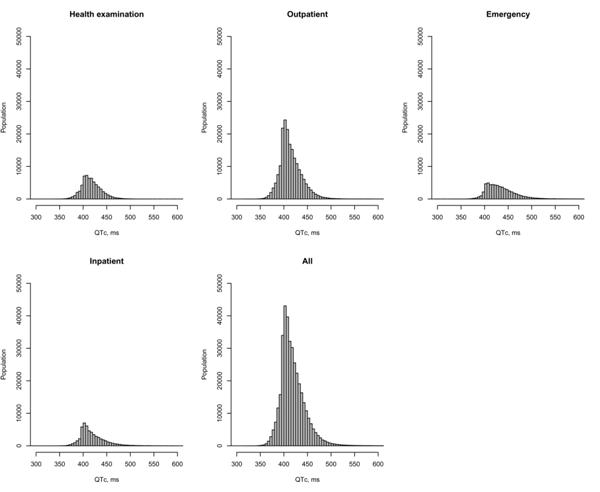
<The QTc distribution and size of study populations in ECG-ViEW
according to the department where the ECG was measured>
The proportion of QTc prolongation (M >450 ms, F >460 ms)
was 8.1%. There were 37.9 million prescriptions
for 911 classes of drugs and 2.9 million laboratory test
results for selected electrolytes (serum potassium, calcium,
and magnesium) during the observation period in ECG-ViEW.
Characteristics of the ECGs by department
About half (44.5%) of ECG recordings
were performed at outpatient departments. QTc prolongation was most
prevalent at emergency departments (25.4%),
followed by inpatient (17.1%), outpatient (7.5%),
and health examination departments (4.1%),
in descending order.
<Characteristics of ECGs in ECG-ViEW by
departments>
|
Variables
|
Department
|
p-value
|
Total
|
|
Health
examination
|
Outpatient
|
Emergency
|
Inpatient
|
|
|
n
|
125794 (17.7%)
|
316158 (44.5%)
|
108802 (15.3%)
|
159615 (22.5%)
|
|
710369 (100%)
|
|
RR interval, ms
|
953.2 ± 138.5
|
850.7 ± 172.4
|
790.9 ± 190.8
|
820.4 ± 191.7
|
<0.001*
|
852.9 ± 181.9
|
|
QT interval, ms
|
406.6 ± 29.0
|
383.6 ± 41.7
|
387.2 ± 50.3
|
385.2 ± 49.8
|
<0.001*
|
388.6 ± 44.0
|
|
QTc interval, ms
|
417.5 ± 20.7
|
417.9 ± 26.4
|
438.8 ± 36.5
|
428.4 ± 36.3
|
<0.001*
|
423.4 ± 30.8
|
|
QTc interval by category, ms
|
|
|
|
|
<0.001†
|
|
|
<390
|
7623 (6.1%)
|
26002 (8.2%)
|
2193 (2.0%)
|
7247 (4.5%)
|
|
43065 (6.1%)
|
|
390
to <420
|
66343 (52.7%)
|
164918 (52.2%)
|
34062 (31.3%)
|
72616 (45.5%)
|
337939 (47.6%)
|
|
420
to <450
|
42934 (34.1%)
|
91558 (29.0%)
|
38824 (35.7%)
|
46961 (29.4%)
|
220277 (31.0%)
|
|
450
to <480
|
7918 (6.3%)
|
26344 (8.3%)
|
21830 (20.1%)
|
20409 (12.8%)
|
76501 (10.8%)
|
|
480
to <500
|
739 (0.6%)
|
4147 (1.3%)
|
5894 (5.4%)
|
5444 (3.4%)
|
16224 (2.3%)
|
|
≥500
|
237 (0.2%)
|
3189 (1.0%)
|
5999 (5.5%)
|
6938 (4.3%)
|
16363 (2.3%)
|
|
QTc prolongation
|
5177 (4.1%)
|
23574 (7.5%)
|
27639 (25.4%)
|
27299 (17.1%)
|
<0.001†
|
83689 (11.8%)
|
Data are
n (%) or mean ± SD.
An individual ECG measurement was
regarded as an observation in this table; thus, a patient with many serial ECG measurements was included multiple times.
QTc prolongation, M >450 ms, F >460 ms
*ANOVA test, †Chi-square test
Study for proof of concept
To prove the usefulness of the database as a
surveillance database for detecting QT prolongation associated with medical
products, we conducted a surveillance study against amiodarone, which is well
known to be associated with QT prolongation.1,2 This drug is listed on the first line of the Drugs with a
Risk of Torsades de Pointes on the Arizona CERT website
(http://www.azcert.org/). For the evaluation, reporting odds ratio (ROR) and proportional
reporting ratio (PRR),3 widely
used data-mining algorithms for ADR signal detection from SRS data, were used.
However, the data in this study were observed instead of reporting data. Thus,
we refer to ROR as observed odds ratio and PRR as proportional observed ratio
hereafter. To calculate them, a two-by-two table was created according to
whether the patient took amiodarone and whether QTc was prolonged.
<Study
for proof of concept: amiodaron and QTc prolongation>
|
Amiodarone
|
All other drugs
|
Overall
|
OOR (CI)
|
POR (CI)
|
|
Prolonged
QTc
|
1876 (N1)
|
50614 (N2)
|
52490
|
5.54
(5.18–5.91)
|
3.19
(3.09–3.30)
|
|
Normal
QTc
|
1754 (N3)
|
261992 (N4)
|
263746
|
|
Overall
|
3630
|
312606
|
316236
|
OOR,
Observed odds ratio; POR, proportional observed ratio; CI, 95% confidence
interval
This
leads to the definition of observed odds ratio and proportional observed ratio
as
Observed
odds ratio = (N1/N3)/(N2/N4)
Proportional
observed ratio = (N1/(N1+N3))/(N2/(N2+N4)),
where
N1:
QTc prolonged after study drug (herein amiodarone) prescription
N3:
QTc not prolonged after study drug prescription
N2:
QTc prolonged after all other drugs (except study drug) prescribed
N4:
QTc not prolonged after all other drugs (except study drug) prescribed
Drugs prescribed within one day before ECG
examination were considered as drugs that could affect ECG parameters. QTc
prolongation was defined as intervals longer than 450 msec for males and 460
msec for females.4 Of the 3,630
ECG records conducted within one day after amiodarone prescription, 1,876 ECG
records showed QTc prolongation. In contrast, of the 312,606 ECG records
conducted within one day after prescription of all drugs other than
amiodarone, 50,614 ECG recordings showed QTc prolongation. The observed odds
ratio and proportional observed ratio were 5.54 (95% confidence interval [CI], 5.18–5.91)
and 3.19 (95% CI, 3.09–3.30), respectively.
ECG-ViEW database specification
The ECG-ViEW database consists of
five data tables and two
reference tables
<Data-table lists and descriptions>
|
Table name
|
Description
|
|
Person
|
Demographic and clinical information about a person
|
|
Electrocardiogram
|
ECG recording for a patient at a certain time
|
|
Drug
|
Drug
prescribed at a certain time
|
|
Diagnosis
|
Diagnosis recorded for
a patient at a certain time
|
|
Laboratory
|
Laboratory
test result for
a patient at a certain time
|
|
DrugCodeMaster
|
Prescription code and name of a drug
|
|
DiagnosisCodeMaster
|
A mapping table between local diagnostic code and ICD-10
code
|
<Table specifications>
|
Table name
|
Field
|
Type, precision
|
Description
|
|
Person
|
personid
|
integer
|
Unique identifier, randomly assigned
|
|
sex
|
boolean
|
1 = Male, 0 = Female
|
|
birthday
|
date
|
Date of birth, randomly shifted within ± 90 days
|
|
ethnicity
|
boolean
|
1 = Korean, 0 = Non-Korean
|
|
Electrocardiogram
|
personid
|
integer
|
Unique identifier, randomly assigned
|
|
ecgdate
|
date
|
Date and time when the ECG was recorded. The date
was shifted from the original date by the same number
of days as were
applied to the patient's birthday.
|
|
RR
|
integer
|
RR interval, ms
|
|
QT
|
integer
|
QT, ms
|
|
QTc
|
integer
|
QTc, ms (by Bazett's formula)
|
|
ACCI
|
integer
|
Age-adjusted Charlson comorbidity index
|
|
ecgdept
|
character (1)
|
E = Emergency, H = Health examination, O = Outpatient, I
= Inpatient
|
|
ecgsource
|
character (1)
|
M = ECG management system, P = scanned paper ECG, E =
EHR
|
|
Drug
|
personid
|
integer
|
Unique identifier, randomly assigned
|
|
drugdate
|
date
|
Date and time when the drug was prescribed. The
date was shifted from the original date by the same number of days as were applied to the patient's
birthday.
|
|
druglocalcode
|
character (8)
|
A system-generated local drug code
|
|
atccode
|
character (7)
|
ATC code, up to level 5
|
|
drugdept
|
character (1)
|
E = Emergency, H = Health examination, O = Outpatient, I
= Inpatient
|
|
route
|
character (1)
|
Route of drug administration, P = parenteral
(injection), E = enteral
|
|
duration
|
integer
|
Duration of drug use
|
|
DrugcodeMaster
|
druglocalcode
|
character (8)
|
Local code for a drug
|
|
igrdname
|
character (50)
|
Drug ingredient
|
|
Diagnosis
|
personid
|
integer
|
Unique identifier, randomly assigned
|
|
diagdate
|
date
|
Date and time when the diagnosis was made. The date was shifted
from the original date by
the same number of days as were applied to the patient's birthday.
|
|
diaglocalcode
|
Character
(8)
|
Local code for diagnosis
|
|
icdcode
|
character(7)
|
ICD-10 code for diagnosis
|
|
diagdept
|
character(1)
|
E = Emergency, H = Health examination, O = Outpatient, I
= Inpatient
|
|
DiagnosisCodeMaster
|
diaglocalcode
|
character (8)
|
Local code for diagnosis
|
|
diagnosis
|
character (190)
|
Diagnosis, full text
|
|
Laboratory
|
personid
|
integer
|
Unique identifier, randomly assigned
|
|
labdate
|
date
|
Date and time when the laboratory sample was drawn
from the patient. The date was shifted from the original date
by the same number of days as were applied to the patient's birthday.
|
|
labname
|
character (1)
|
1 = serum potassium, 2 = serum magnesium, 3 = serum
calcium
|
|
labvalue
|
number (7,2)
|
Laboratory test result
|
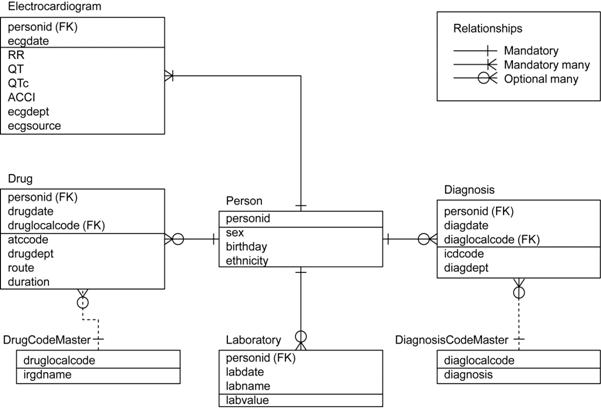
<The entity-relationship diagram (ERD) for the ECG-ViEW data tables
and their relationships>
Comparison with previous studies
Although the literature regarding QT intervals
is substantial, there are no standards for distribution of QT intervals in the
population. Based on the criteria presented in previous studies, the average
QTc of ECG-ViEW was similar to that of an English study that evaluated 3,596
older (60–79 years) participants.5
However, it was longer than that reported in a Finnish study involving 10,822
participants.6 QTc
prolongation in ECG-ViEW was comparable to, or less than, that in a Dutch study
(390 patients)7 or the English
study noted above. The average QTc in ECG-ViEW was between two US studies
involving 7,828 participants aged 40 years or older8 and 46,129 normal volunteers.9 The differences may result from differences in the
ethnicity and/or study populations among the study groups. Only ECG-ViEW
contains associated clinical data and is open access, in contrast to the
previous studies and ECG databases.
<Comparison
of ECG-ViEW with previous studies>
|
Study
|
Country
|
Population type
|
ECG type
|
HR correction formula
|
Age, years
|
No. of subjects
|
Gender
|
QTc, ms
|
QTc prolongation
|
|
Criteria, ms
|
Proportion
|
|
Zhang8
|
U.S.
|
general
|
Standard*
|
Bazett
|
≥40
|
7828
|
-
|
429 ±
23
|
-
|
-
|
|
ECG-ViEW
|
Korea
|
HE
|
37376
|
-
|
420 ±
22
|
-
|
-
|
|
Algra7
|
Netherlands
|
patient
|
Ambulatory†
|
Bazett
|
-
|
390
|
-
|
-
|
≥440
|
0.22
|
|
ECG-ViEW
|
Korea
|
patient
|
Standard
|
308825
|
-
|
-
|
≥440
|
0.19
|
|
Sohaib5
|
England
|
general
|
Standard
|
Hodge
|
60–79
|
3596
|
-
|
419 ±
26
|
>440
|
0.19
|
|
>500
|
0.01
|
|
ECG-ViEW
|
Korea
|
HE
|
6397
|
-
|
424 ±
22
|
>440
|
0.21
|
|
>500
|
0.01
|
|
Anttonen6
|
Finland
|
general
|
Standard
|
Bazett
|
30–59
|
10822
|
M
|
402 ±
54
|
-
|
-
|
|
F
|
415 ±
52
|
|
ECG-ViEW
|
Korea
|
HE
|
52160
|
M
|
411 ± 19
|
-
|
-
|
|
F
|
424 ± 20
|
|
Mason9
|
U.S.
|
general
|
Standard
|
Bazett
|
-
|
46129
|
M
|
401 (median)
|
≥449
|
0.02
|
|
F
|
414 (median)
|
≥460
|
0.02
|
|
ECG-ViEW
|
Korea
|
HE
|
62576
|
M
|
409 (median)
|
≥449
|
0.04
|
|
F
|
422 (median)
|
≥469
|
0.06
|
Data are
n (%) or mean ± SD
*Standard resting 12-lead ECG
†24-hour ambulatory ECG
ECG, Electrocardiogram; HR, heart rate; HE, health examination
REFERENCES
1. Riera, A.R., et al. Relationship among amiodarone,
new class III antiarrhythmics, miscellaneous agents and acquired long QT
syndrome. Cardiol J 15, 209-219 (2008).
2. Taira, C.A., Opezzo,
J.A., Mayer, M.A. & Hocht, C. Cardiovascular drugs inducing QT
prolongation: facts and evidence. Curr
Drug Saf 5, 65-72 (2010).
3. Brian L. Strom,
S.E.K. textbook of pharmacoepidemiology,
(John Wiley & Sons Ltd, Chichester, 2006).
4. Rautaharju, P.M., et al. AHA/ACCF/HRS recommendations for
the standardization and interpretation of the electrocardiogram: part IV: the
ST segment, T and U waves, and the QT interval: a scientific statement from the
American Heart Association Electrocardiography and Arrhythmias Committee,
Council on Clinical Cardiology; the American College of Cardiology Foundation;
and the Heart Rhythm Society. Endorsed by the International Society for
Computerized Electrocardiology. J Am Coll
Cardiol 53, 982-991 (2009).
5. Sohaib, S.M.,
Papacosta, O., Morris, R.W., Macfarlane, P.W. & Whincup, P.H. Length of the
QT interval: determinants and prognostic implications in a population-based
prospective study of older men. J
Electrocardiol 41, 704-710
(2008).
6. Anttonen, O., et al. Prevalence and prognostic
significance of short QT interval in a middle-aged Finnish population. Circulation 116, 714-720 (2007).
7. Algra, A., Tijssen,
J.G., Roelandt, J.R., Pool, J. & Lubsen, J. QTc prolongation measured by
standard 12-lead electrocardiography is an independent risk factor for sudden
death due to cardiac arrest. Circulation
83, 1888-1894 (1991).
8. Zhang, Y., et al. QT-interval duration and
mortality rate: results from the Third National Health and Nutrition
Examination Survey. Arch Intern Med 171, 1727-1733 (2011).
9. Mason, J.W., et al. Electrocardiographic reference
ranges derived from 79,743 ambulatory subjects. J Electrocardiol 40,
228-234 (2007).


